Uncover the deeper layers of gout as Dr. Naomi Schlesinger walks through our current understanding of gout pathophysiology and an integrated approach to managing gout flares in this engaging video:
What percentage of patients with gout are undermanaged?
Gout is a complex disease, and managing gout flares requires HCPs to have a deeper understanding of the underlying interplay of inflammatory pathways.2
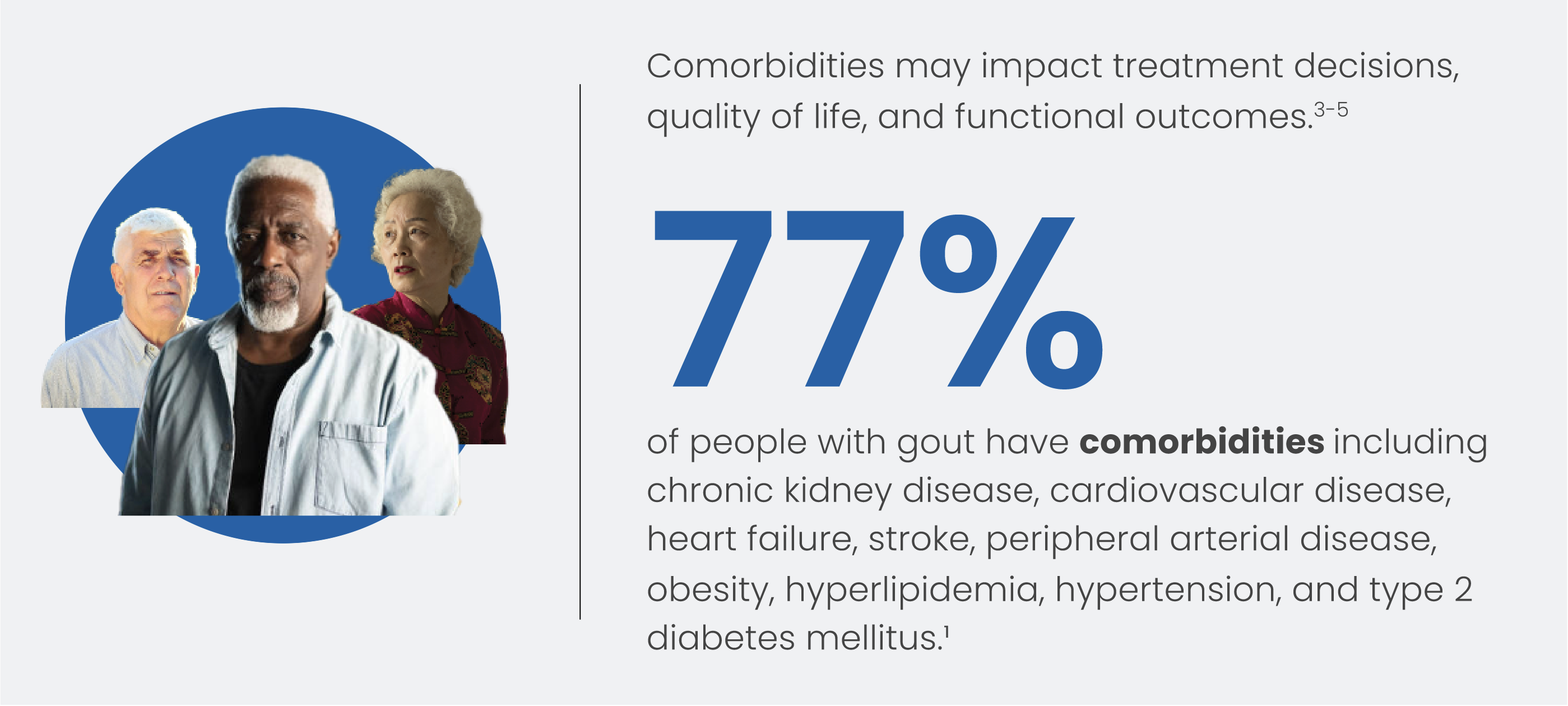
Comorbidities
Pathophysiology
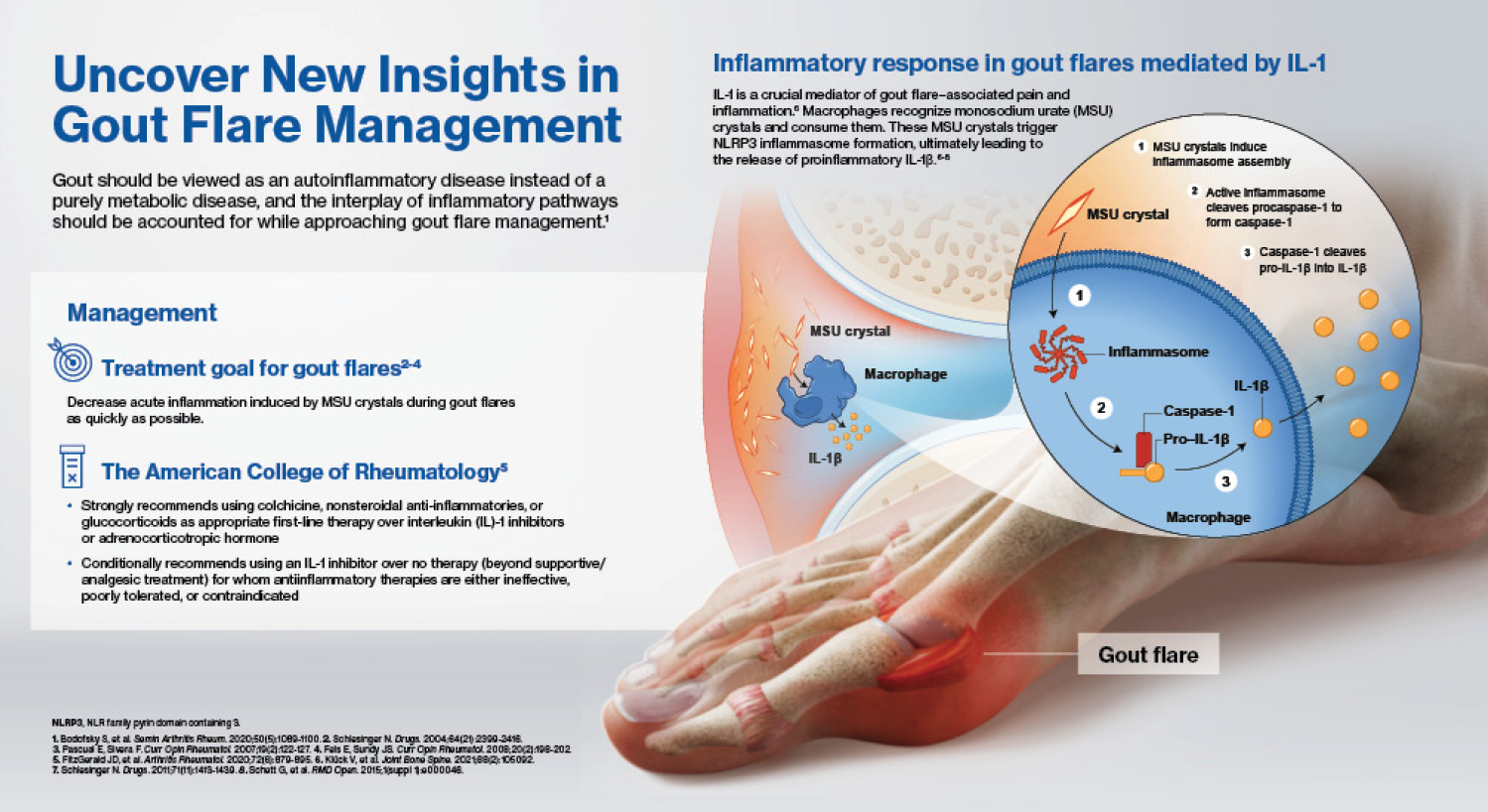
Gout should be viewed as an autoinflammatory disease instead of a purely metabolic disease.2,3
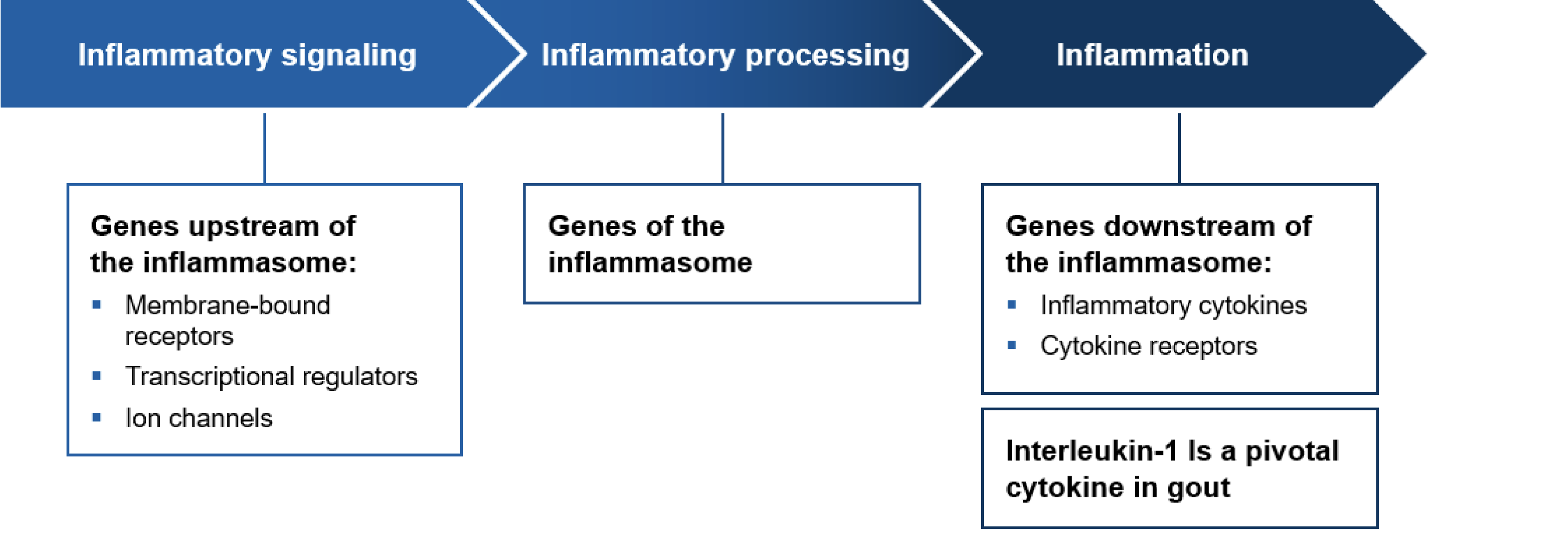
At the molecular level
Adapted with permission from Schlesinger et al.3
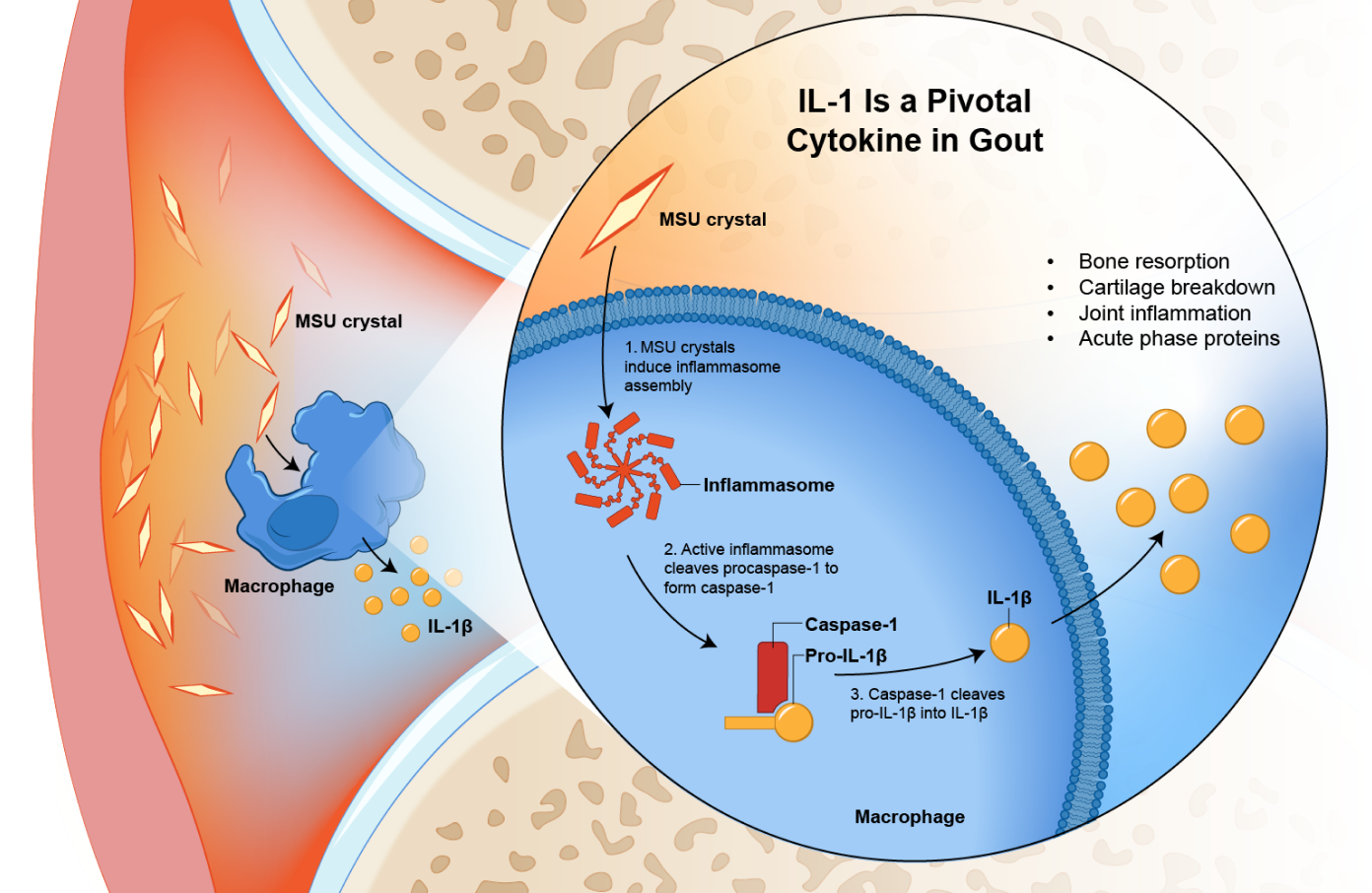
Gout flares depend on 2 switches3,6,7:
- The activation of the TLR2/4–NF-kB signaling pathway that promotes the synthesis of pro–IL-1β and significant components of the inflammasome
- Stimulating sodium urate crystals activates the NLRP3 inflammatory pathway by promoting the assembly of inflammatory vesicles, thereby promoting the conversion of pro-caspase-1 to caspase-1. This leads to the conversion of pro-IL-1β to the proinflammatory IL-1β via caspase 1, followed by the release of IL-1β
IL-1β acts as a proinflammatory mediator—inducing vasodilation, recruitment of additional leucocytes, and the expression of proinflammatory cytokines and chemokines.
Management
An integrated approach to treatment
Nonpharmacological factors also play an important role in managing gout flares

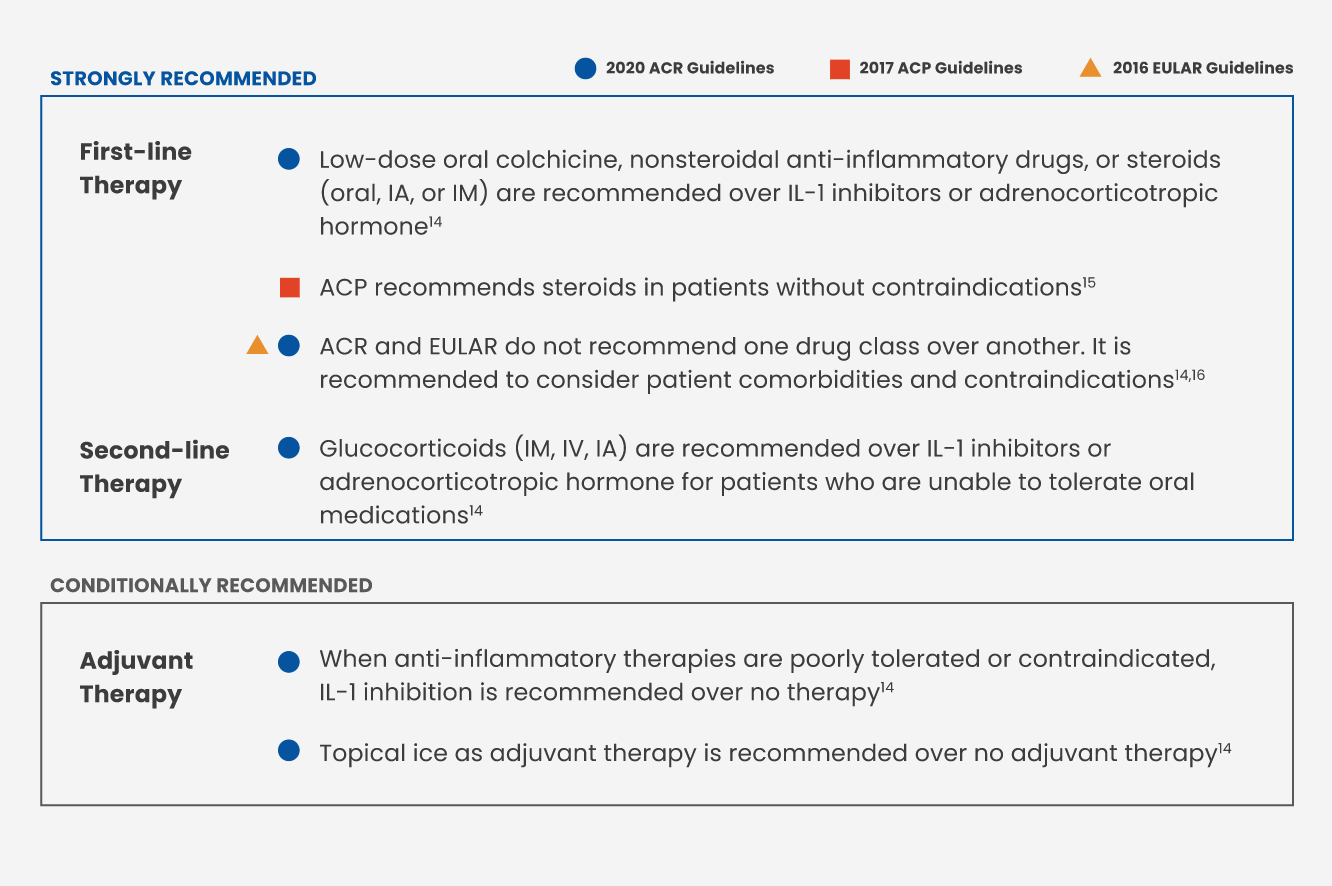
Treatment goal for gout flares11-13
Decrease acute inflammation induced by MSU crystals during gout flares as quickly as possible.
ACR 2020 Standard of Care Treatment Guidelines: Latest updates in treating gout flares
Unmet needs in effective acute and chronic gout management17,18

Summary
Review this synopsis of our current understanding of the pathophysiology and management of gout flares
Abbreviations:
ACP, American College of Physicians; ACR, American College of Rheumatology; EULAR, European Alliance of Associations for Rheumatology; HCP, health care professional; IA, intra-arterial;
IL, interleukin; IM, intramuscular, IV, intravenous; MSU, monosodium urate; NF-kB, nuclear factor kappa-light-chain-enhancer of activated B cells; TLR, toll-like receptor.
References:
1. De Meulemeester M, et al. BJGP Open. 2020:1-9. 2. Bodofsky S, et al. Semin Arthritis Rheum. 2020;50(5):1089-1100. 3. Schlesinger N. Drugs. 2011;71(11):1413-1439. 4. Bardin T, Richette P. BMC Med. 2017;15:123. 5. Singh JA. Curr Rheumatol Rep. 2009;11(2):154-160. 6. Luo Z, et al. Front Endocrinol (Lausanne). 2022;13:967769. 7. Zhao J, et al. Front Immunol. 2022;13:888306. 8. Piillinger MH, Mandell BF. Semin Arth Rheum. 2020;50:S24-S30. 9. Fields TR. Rheum Dis Clin N Amer. 2019(45):145-157. 10. Fitzgerald J et al. Arthritis Care Res (Hoboken). 2020;72(6):744-760. 11. Schlesinger N. Drugs. 2004;64(21):2399-2416. 12. Pascual E, Sivera F. Curr Opin Rheumatol. 2007;19(2):122-127. 13. Fels E, Sundy JS. Curr Opin Rheumatol. 2008;20(2):198-202. 14. FitzGerald JD, et al. Arthritis Rheumatol. 2020;72(6):879-895. 15. Qaseem A, et al. Ann Intern Med 2017;166(1):58-68. 16. Richette P, et al. Ann Rheum Dis. 2017;76(1):29-42. 17. De Vera MA et al. Arth Care Res. 2014;66(10):1551-1559. 18. Perez-Ruiz F, Desideri G. Ther Clin Risk Manag. 2018;14:793-802.